Saving lives or saving the economy?
In this article, Robert Östling argues that the polarizing debate over the choice of saving lives or saving jobs may be misleading. He describes different options for policymakers and how we can understand why countries have chosen alternative strategies. The conclusion is that the COVID-19 pandemic has shown how economic and epidemiological aspects are more intertwined than previously thought.
The policy response to the COVID-19 pandemic has spurred a polarized debate around the globe. At one end of the debate, it has been argued that the drastic lockdowns undertaken by many countries constitute an overreaction that hurts the economy and that the cure may turn out to be worse than the disease. At the other end of the debate, it has been argued that we must do all we can to try to save as many lives as possible. Sweden has chosen a different policy than many other countries and “the Swedish model” has appeared as a rhetorical weapon in the debate. Many see the policy choice as a choice between saving lives and saving the economy and Sweden’s policy is sometimes taken as a sign that Sweden puts greater weight on economic considerations than other countries. But the trade-off between money and lives need not be as sharp as many believe, and perhaps can be avoided altogether.
The Swedish COVID-19 policy is not spelled out clearly in official documents, but it is apparent that a priority is to ensure that the health care system does not risk becoming overburdened. This policy objective can be illustrated using an epidemic curve which shows how people during an epidemic are infected at increasing speed until so many are infected that spreading starts to slow down. After the turning point, there are fewer newly infected for every day and eventually the infection dies out. If the peak of the curve is too high, there will be too many that simultaneously need health care which will lead to excess deaths and suffering. This is illustrated in Figure 1 below. The steep red curve shows the number of newly infected during an uncontrolled epidemic and the horizontal dashed line shows health care capacity. The area between the red curve and the dashed line shows the number of patients that will not get appropriate medical treatment.
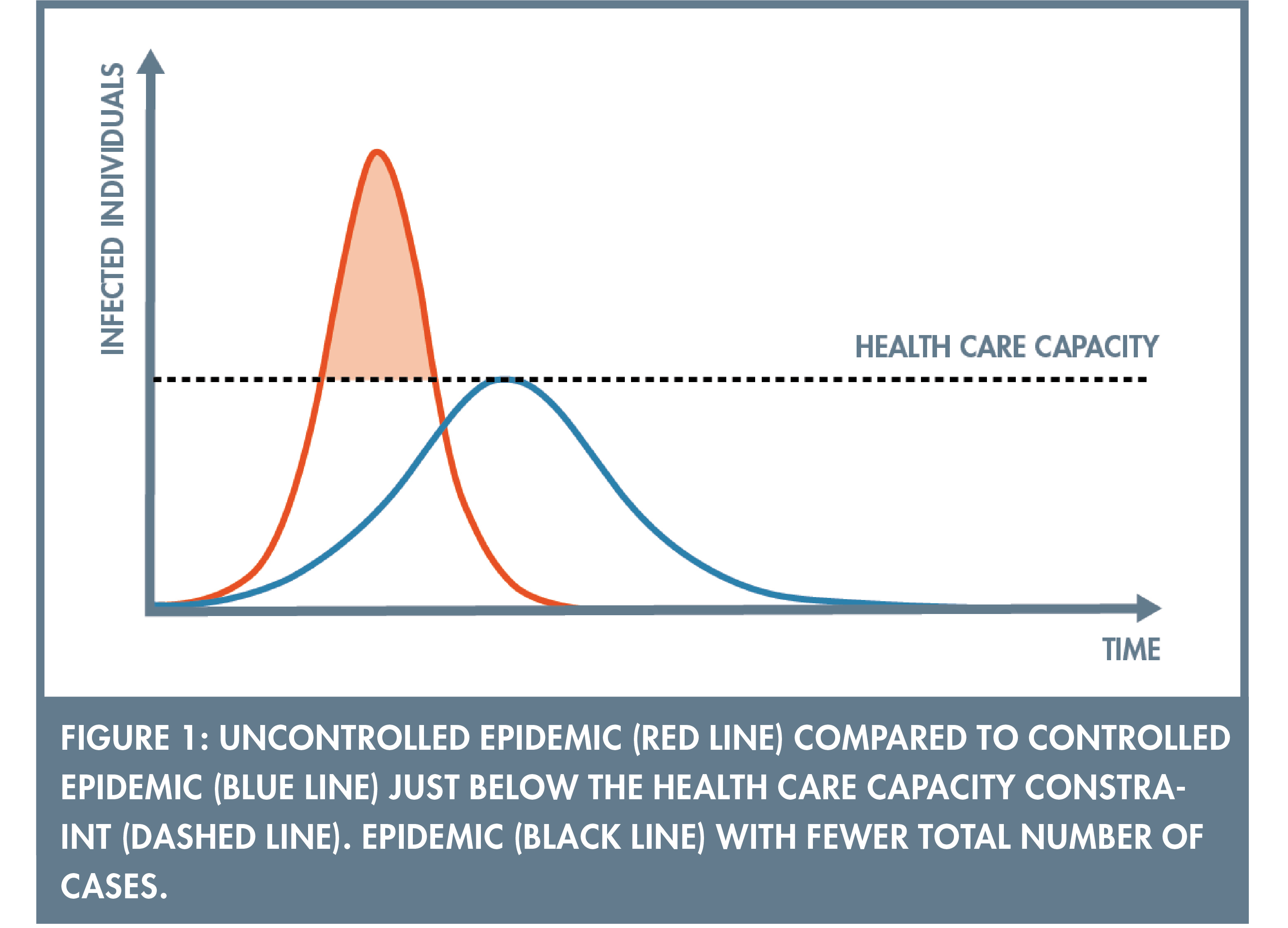
To avoid unnecessary deaths, policymakers can take measures to limit how quickly the disease is spreading and thereby “flatten the curve”. The case where the curve is sufficiently flattened so that the number of infected is just below health care capacity is illustrated by the flatter blue line in Figure 1. Unfortunately, the policies that limit contagion are also likely to reduce both production and consumption. Under the most extreme policy, complete lockdowns, workers cannot go to work and consumers cannot shop (apart from groceries and medicines). But less drastic measures, such as restricting public gatherings, are also likely to hurt at least some sectors of the economy. In this simple framework, policymakers hence face a trade-off between reducing the size of the red area to avoid unnecessary deaths and to keep the economy going.
To make that trade-off optimally, policymakers need an assessment about how many lives that would be lost in an uncontrolled epidemic (corresponding to the size of the red area in Figure 1). A report published on March 16, 2020 by a large team of scientists led by the British epidemiologist Neil Ferguson appears to have had a very large impact in shaping the perception about the consequences of exceeding health care capacity during the COVID-19 pandemic (1). The report provided estimates for the UK and the US and estimated that 510,000 people in the UK could die in an uncontrolled pandemic. The UK has a population of 66 million, so rescaling those numbers for Sweden suggests that some 77,000 Swedes would die in an uncontrolled pandemic.
Many would probably conclude from such numbers that no further analysis is needed. The fact that we are risking so many people’s lives means that we must make sure not to exceed health care capacity. But we can also use conventional cost-benefit analysis to help us make the trade-off. Policymakers routinely make decisions about population health and there are standards for how lives are valued, for example when deciding how much to invest in road safety. Such assessments are often expressed as the value of saving one quality-adjusted year of life (QALY), i.e. the monetary value attached to reducing mortality risk so that one additional year of a healthy individual’s life is saved. These valuations are not used at the individual level, for example when deciding whether a specific individual should be given an expensive medical treatment. But they are used in cost-benefit analyses when deciding on alternative policies that change mortality risks in a population. One estimate that is sometimes used in Sweden is around 1 million SEK per QALY.
Suppose that each COVID-19 death on average leads to five to ten healthy years lost. Under this assumption, 77,000 lives correspond to somewhere between 385,000 and 770,000 QALYs. In economic terms this corresponds to 385 to 770 billion SEK, or 8 to 15 percent of GDP. These estimates suggest that the price worth paying for not exceeding health care capacity is very high also using standard methods for valuing lives. The National Institute of Economic Research forecasted in May 2020 that Swedish GDP would fall by 7 percent during 2020, so judging from this forecast Sweden implicitly appears to make an economic sacrifice of a similar order of magnitude as the cost-benefit computations suggest.
This calculation merely serves to illustrate order of magnitudes and it does not consider that not all those 77,000 lives can be saved. There is also a lot of uncertainty in projecting the consequences of an uncontrolled pandemic. Ferguson’s report has been criticized for being overly pessimistic and may not withstand the test of time. But if these estimates reflect expert assessments available in March 2020, it is easy to understand why so many countries undertook drastic measures to reduce the spread of the disease. Leading academic economists were also quick to support such policies. The IGM Forum at the Chicago Booth School of Business routinely surveys a panel of world-leading academic economists about their attitudes to various public policies. Among the economists surveyed in late March 2020, there was nearly unanimous support for the statement that “a comprehensive policy response to the coronavirus will involve tolerating a very large contraction in economic activity until the spread of infections has dropped significantly.”
Whereas there is strong agreement about not exceeding health care capacity, there is more controversy regarding whether the epidemic curve should be pushed further below the health care capacity constraint. The red and blue curves in Figure 1 are drawn so that the area under both curves is the same, i.e. the total number of infected is the same irrespective of how quickly the disease is spreading. Former Swedish state epidemiologist, Johan Giesecke, seems to be of this opinion according to a letter to the medical journal Lancet on May 5, 2020: “I expect that when we count the number of deaths from COVID-19 in each country in 1 year from now, the figures will be similar, regardless of measures taken.” But this is a controversial view. Many argue that further flattening the curve will result in a lower total number of infected and fewer deaths. This situation is depicted by the black line in Figure 2.
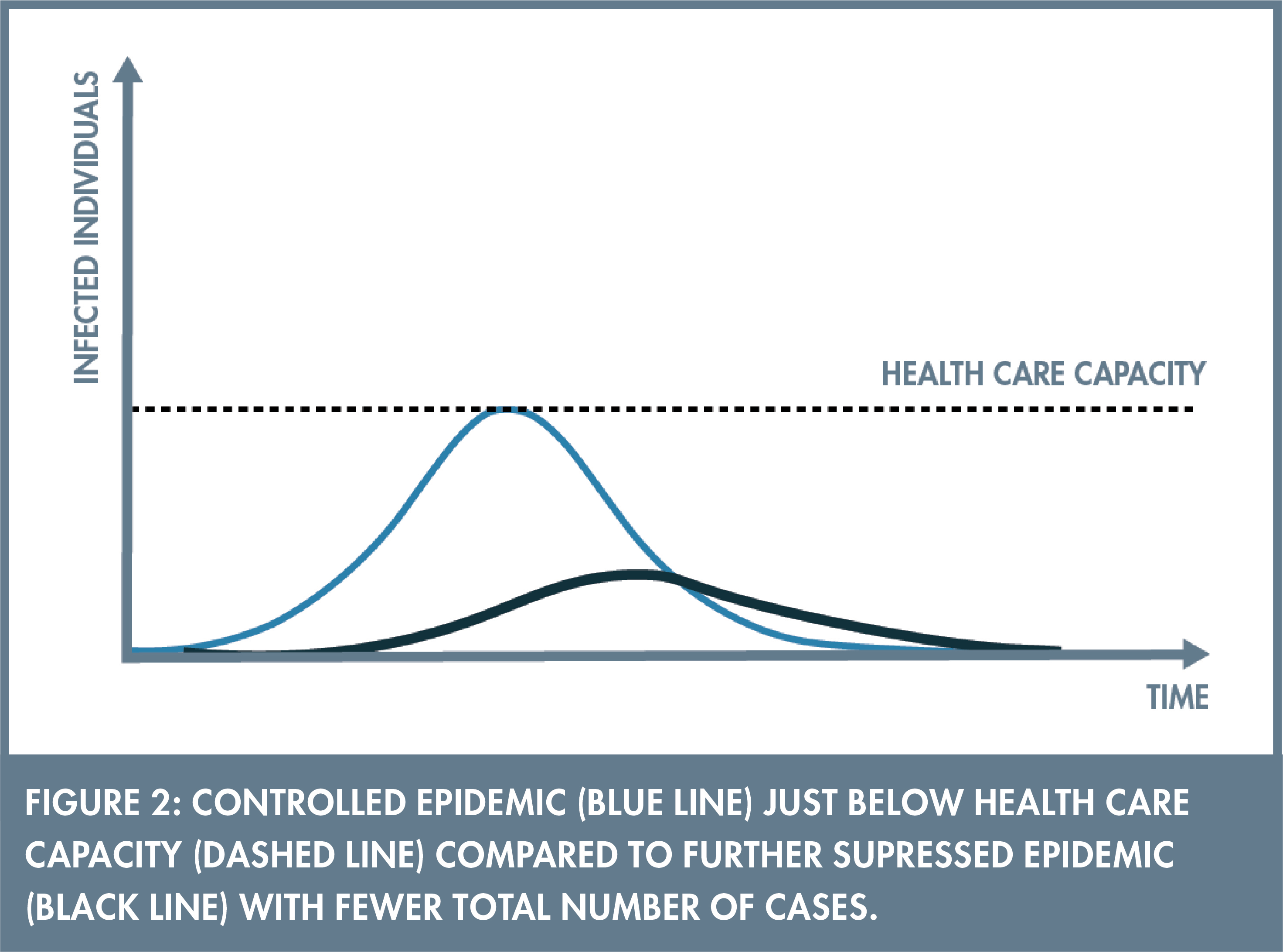
There are several reasons why the total number of infected may be lower if the disease spreads more slowly. One possibility is that the black line in Figure 2 is pushed all the way down to the horizonal axis so that the virus is eliminated. But also less drastic measures may save lives. For example, the possibility that a vaccine arrives means that lives will be saved if the population has not already reached herd immunity when the vaccine becomes available. There are also other reasons why postponing the peak of the epidemic may save lives, for example if it buys time to expand health care capacity, to increase testing capacity or to learn about medical treatment of the disease.
Another reason why a flatter curve may save lives comes directly from a simple epidemiological model, the SIR model. A common assumption is that absent policies to limit contagion, every infected individual spreads COVID-19 to on average 2.5 other individuals. This implies that at least 60 percent need to get infected to reach herd immunity. But an uncontrolled pandemic can result in as many as 90 percent getting infected. The reason is that the disease spreads so quickly at the peak of the pandemic that the virus naturally “overshoots” the herd immunity threshold.
There is however also a potential risk associated with postponing the pandemic. If resources are exhausted too early, a second or third wave of the virus may have larger impact compared to a country that has already built up some immunity in the population.
Different countries have chosen to go to different lengths in limiting contagion. Two extremes are Sweden and New Zealand. Up until May 31, Sweden had reported 4,415 deaths. At its peak in April 2020, at least in Stockholm County, the pandemic appears to have been very close to the health care capacity constraint. At that time, there were more than 200 people treated in intensive care units in Stockholm, which is more than twice as many intensive care units than are normally available. Although Swedish policymakers have denied that they deliberately aimed to build up herd immunity, they have acknowledged that it may be a consequence of the policy. At the other extreme, New Zealand has decided to try to eliminate the virus altogether. Up until May 31, only 26 deaths had been reported, in a country with a population half the size of Sweden. Although the two countries have implemented different policies, there are of course also many other potential explanations for the different outcomes in the two countries.
Most other countries are found somewhere in between these extremes both in terms of the policies implemented and death tolls. But how much should policymakers invest in further limiting the spread of COVID-19 below the health care capacity constraint? One option is to seek guidance from the type of cost-benefit analysis discussed above. For example, if 60 percent of Sweden’s population is eventually infected and the infection mortality rate is 0.6 percent, then 36,000 lives might be lost during the pandemic. In monetary terms going through the same rough calculations as above, this corresponds to 4 to 7 percent of Swedish GDP. The policies that would be required to flatten the curve further is likely to reduce consumption and production and would have to be in place for a long period of time and that cost may very well be higher than a few percent of GDP.
This line of reasoning again puts the policy choice mainly as a trade-off between money and lives. There are however good reasons to believe that the policy choice need not involve such a sharp trade-off. One reason is that some of the reduction in labor supply and consumption following lockdowns may occur also without social distancing policies. When the disease is spreading quickly, especially if health care capacity is exceeded and people realize they might not get adequate treatment, people react by cutting down consumption and abstaining from work in order to avoid getting infected. This also means that public policies that limit contagion might serve the dual goal of saving lives and getting more people back to work. It is well-known from previous epidemics that people spontaneously engage in social distancing and there is evidence suggesting that social activity in both the US and Sweden in March 2020 declined prior to the implementation of social distancing policies (2). Preliminary research using data from US cities during the 1918 influenza pandemic finds that there is no evidence that cities that implemented more restrictive policies fared worse economically, but on the other hand no evidence to the contrary either (3).
Several economists have also argued that the trade-off between money and lives can be alleviated substantially by radically expanding testing capacity, perhaps combined with digital tracing. For example, Nobel laureate Paul Romer has suggested that we should invest massively in testing so that 10 percent of the population can be tested daily. Romer and his co-authors argue that this would be enough to both keep the pandemic at a very low level and to save the economy because everybody that are not tested positive can continue with their regular lives (4). Similarly, if it is possible to eliminate the virus and then lift restrictions, like New Zealand has been trying to do, then it has clear economic and health advantages.
There is currently a flood of academic papers in economics that develop models combining epidemiological and macroeconomic models to incorporate the different mechanisms discussed above (see e.g. 5). It is easy to make fun of the exponential growth of such papers, but these papers did not appear in a vacuum. Economists have long combined economic and epidemiological models (see 6 for one example) and there is also an epidemiological literature studying optimal policy. But the COVID-19 pandemic has shown that the economic and epidemiological aspects are more intertwined than many previously thought and that the policy choice is complicated and involves epidemiological, economic as well as behavioral considerations.
Economists will most likely continue to analyze what the optimal policy during spring of 2020 should have been long after the COVID-19 pandemic is over. At the time of writing we do not know whether most governments overreacted or whether the response was appropriate. What we do know is that Sweden, at least temporarily, chose a different strategy than many other countries. What we also know is that we learn very little if all governments implement the same policy at the same time. There is a value in policy experimentation and for better or worse, Sweden’s alternative policy response provides data that other countries can learn from.
References
(1) Ferguson, N., Laydon, D., Nedjati Gilani, G., Imai, N., Ainslie, K., Baguelin, M., ... & Dighe, A. (2020). Report 9: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand.
(2) Farboodi, M., Jarosch, G., & Shimer, R. (2020). Internal and external effects of social distancing in a pandemic (No. w27059). National Bureau of Economic Research.
(3) Lilley, A., Lilley, M., & Rinaldi, G. (2020). Public health interventions and economic growth: Revisiting the Spanish flu evidence. Available at SSRN 3590008.
(4) Taipale, J., Romer, P., & Linnarsson, S. (2020). Population-scale testing can suppress the spread of COVID-19. medRxiv.
(5) Eichenbaum, M. S., Rebelo, S., & Trabandt, M. (2020). The macroeconomics of epidemics (No. w26882). National Bureau of Economic Research.
(6) Kremer, M. (1996). Integrating behavioral choice into epidemiological models of AIDS. The Quarterly Journal of Economics, 111(2), 549-573.

Robert Östling is Associate Professor of Economics at the Department of Economics at Stockholm School of Economics.